
Written by Tiffany Lillie, Senior Technical Advisor, LINKAGES
The USAID– and PEPFAR-supported LINKAGES project aims to increase the number of key population (KP) members who are tested for HIV and who begin and remain in treatment after testing positive. To accomplish this, programs need to (1) expand HIV testing services, (2) effectively link people who test positive into care and treatment, and (3) re-engage HIV-positive individuals who have dropped out of care and link them back to treatment services.
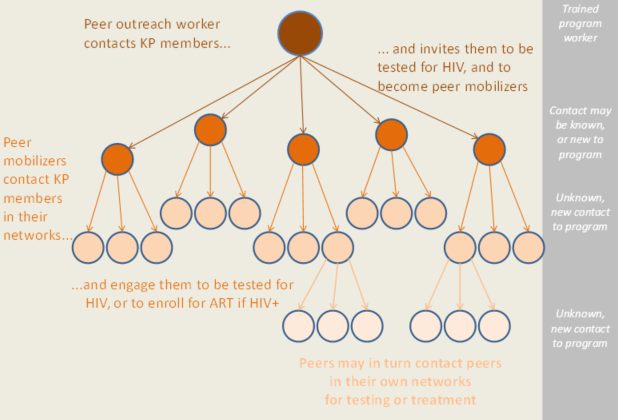
To address the challenge of expanding outreach to KP members, USAID and FHI 360 developed the enhanced peer outreach approach (EPOA). The EPOA is led by peer outreach workers, who are trained to create and manage a “referral chain network.” This network has at least three levels. The first level is the peer outreach workers (usually KP members), who are trained to engage new KP members in HIV testing and to identify other KP members to serve as “peer mobilizers.” Peer mobilizers, the second level in the referral chain network, have undergone HIV testing (and, if HIV positive, are enrolled in treatment); they pass referral slips for HIV testing to members of their social or sexual networks. The third level of the referral chain are these peers referred by peer mobilizers to testing or antiretroviral treatment. If peers at this level get tested or visit a facility for treatment, both the peer mobilizer and peer outreach worker can receive a small incentive.
EPOA’s referral chain network
The EPOA empowers entire KP groups to be actively involved in improving HIV-related health outcomes for themselves and their communities. And by reaching deeper into social and sexual networks than is possible through traditional peer outreach, the EPOA is able to engage previously unidentified, high-risk, hard-to-reach KP members, particularly those who are not found at traditional locations (for example, bars and clubs, parks, and brothels).
To support countries in using the EPOA, LINKAGES developed the Enhanced Peer Outreach Approach (EPOA) Implementation Guide and will soon be releasing an accompanying training guide.
The EPOA is currently being scaled up by LINKAGES partners in several countries in Asia, Africa, and the Caribbean. Thus far, HIV case findings have shown improvements in all communities with one or more KP groups. In Burundi, for example, 2,451 referral slips were distributed to female sex workers (FSWs) during a nine-week pilot. Out of 929 (37.9%) FSWs tested, 100 (11%) of them were found to be HIV positive and 90 (90%) of those were initiated into treatment. The average HIV-positive yield of 11% represents an increase over the 5% HIV-positive yield found in the three months prior to the introduction of the EPOA.
Henriette Manishimwe, project coordinator for the Society for Women Against AIDS in Africa-Burundi, shares her initial thoughts:
“The EPOA not only helped increase HIV testing yield, but also the demand for other services like sexually transmitted infection screening and treatment. It [has also provided] an opportunity to increase our index testing, because all positive FSWs who have young children got them tested.”
While data are preliminary, this demonstrates the potential effectiveness of the EPOA in identifying those who are HIV-positive and initiating them into treatment. Widespread implementation of the EPOA with high-risk populations holds promise as a strategy that could accelerate progress toward UNAIDS’ 90-90-90 targets.