
Benjamin Eveslage, Technical Advisor, Online HIV Services, FHI 360
This blog post was originally published here on PSI’s website.
The global response to HIV is now threatened on many fronts: insufficient funding, myriad challenges posed by COVID-19, and slow adoption of new HIV service technologies and delivery methods. UNAIDS now reports inequitable progress and recent setbacks in many countries. Putting HIV services and care in the hands of individuals will be part of the solution.
Community advocates, researchers, and HIV program implementers met virtually this year for the AIDS 2020: Virtual conference and discussed innovations and adaptations to help address these challenges — highlighting the conference’s theme of “resilience.” Approaches and technologies that allow people to direct and support their own HIV care—with or without a provider—was a critical topic emerging from the conference. Let’s call this “doing it yourself” or “self-care” — defined by the World Health Organization in their first normative guidance on self-care interventions for health published in 2019.
Why is self-care required to respond to HIV?
-
PEOPLE LIKE “DOING IT” THEMSELVES!
Getting HIV under control means ensuring that people living with HIV know their HIV status, start antiretroviral treatment (ART), and reach viral suppression to prevent onward transmission (see UNAIDS 95-95-95 targets). However, clinic- and provider-based services are not a one-size-fits-all approach. Clients who want more privacy or autonomy when accessing health care are often left out. For example, key populations most affected by HIV may avoid services because of perceived and experienced stigma and discrimination in health settings.
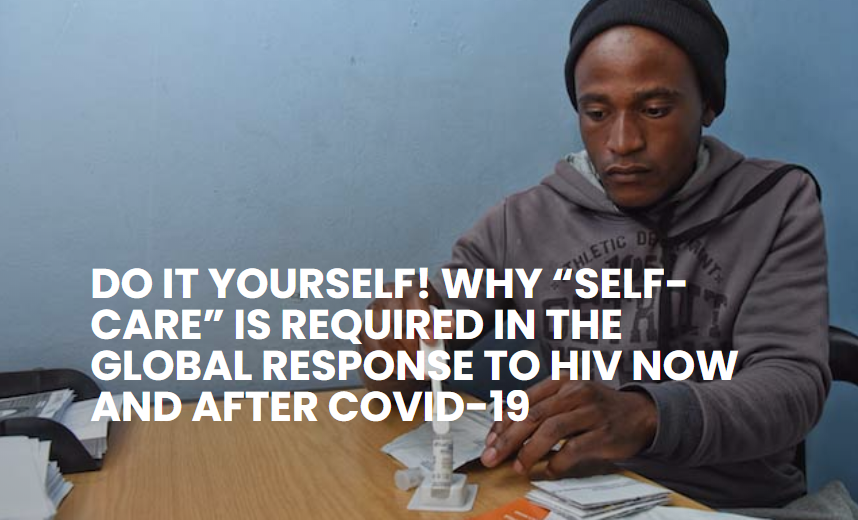
But what can people really do themselves? HIV self-testing, for one. Testing technology has advanced over the years to make self-testing possible along with rapid policy change and implementation across various countries. For example, the STAR project in Southern Africa distributed more than 4.8 million HIV self-test kits between 2015 and 2019. The COVID-19 pandemic is accelerating rollout of HIV self-testing. HIV self-testing satisfies people’s preference for autonomy and privacy, and it is especially useful for people in settings where traditional HIV testing was limited. Young people are another important demographic for self-testing: they experience more stigma accessing sexual health services and may already be accustomed to using a whole range of at-home options from food delivery to virtual family chats. Self-care is easily marketed to target audiences directly and also championed by social media influencers who can “make HIV-related self-care famous.”
Self-care does not end at HIV testing: HIV programs may also support clients to manage their own use of pre-exposure prophylaxis (PrEP) (see on-demand PrEP), self-sampling for sexually transmitted infections, and several other self-care approaches.
-
PEOPLE STAY HOME, MAINTAIN SAFE DISTANCE, AND REDUCE BURDEN ON HEALTH WORKERS
Supporting clients to “do it” on their own, means health workers may be “doing it” less. The resulting time and cost savings can be used to optimize the health system’s capacity to respond to HIV and COVID-19. Where to start? There are lots of options! For example, multimonth ART refills plus home delivery and virtual case management can be implemented to support uninterrupted ART and allow people living with HIV to take greater ownership of their HIV care, remain at home, and reduce unnecessary health facility visits.
COVID-19 will affect the provision of HIV services well into the future. The USAID- and PEPFAR-funded LINKAGES project in Jakarta, Indonesia is an example of how services are adapting. From March to June 2020, the project supported 47% of all PLHIV enrolled on ART in Jakarta to move from 1-month to 2-month dispensing of ART and 17.6% to receive home delivery. To support this transition, all project-funded case mangers shifted to working with PLHIV through virtual platforms.
-
TO BETTER ENGAGE THE GROWING MOBILE GENERATION
Self-care and digital platforms are a perfect pair: HIV services readily available for people to access on their own through their mobile phone, social media, and the internet.
Currently, about half the world’s population are active social media users, 59% are online, and 67% are using a mobile phone (see Digital 2020 report). This ever-growing trend is forcing change in many HIV programs that are losing contact with, and relevance among, this growing mobile generation. In 2018, FHI 360 supported the development of several interventions for going online to accelerate the impact of HIV programs. The Online Reservation App (ORA) was a critical innovation developed in 2017, and is now used by the ACCELERATE project in India for about 1,000 clients per month to book and access lab-based HIV testing on their own (see Yes4Me.net). ORA also is now used in 11 other countries and was re-launched in 2020 as “QuickRes” as a multicountry platform. Digital technology is a critical enabler for self-care, because people already use the internet and social media to learn about available HIV services they can use on their own.
To get the HIV response back on track, self-care models must supplement traditional clinic- and provider-led models. Even before the COVID-19 pandemic, in-person service delivery was not the preferred approach for some people, and now we live in a new world where in-person services are potentially dangerous. It’s time to recognize and embrace this change and build #better4tomorrow.
This post summarizes an AIDS 2020 satellite session “Bringing Self-Care into the HIV Response” hosted by The Self Care Trailblazer Group, Children’s Investment Fund Foundation, Population Services International, International Planned Parenthood Federation, PATH, FHI 360, Jhpiego, and Aidsfonds.